Knee Osteoarthritis: Causes, Symptoms & Treatment Options
Knee osteoarthritis (OA) is often seen as an inevitable part of aging, but modern orthopedics has moved beyond the simplistic “wear and tear” narrative. Today, specialists view the knee as a complex system made up of cartilage, bone, synovium, ligaments, and muscle, each influencing the other.
In a healthy knee, cartilage, bone, synovium, and ligaments work together to keep movement smooth and pain-free. OA represents a fundamental failure of this system. It is a progressive degenerative disorder where the biological, chemical, and mechanical environments of the joint are altered. Osteoarthritis is one of the most common causes of chronic pain and disability and can significantly reduce quality of life, influencing everything from career longevity to the simple ability to walk through a grocery store.
According to the Centers for Disease Control and Prevention (CDC), osteoarthritis affects over 32.5 million adults in the United States. The knee, bearing the brunt of our daily vertical load, is the most frequently affected joint. Today, OA is understood as a condition that involves low-grade inflammation alongside mechanical wear. It involves a cascade of events that ripples through the entire joint structure:
- Cartilage Breakdown: The loss of hyaline cartilage, which serves as the joint’s essential, friction-free shock absorber.
- Subchondral Bone Remodeling: The bone beneath the cartilage thickens (sclerosis) and develops “spurs” as it tries to compensate for the lost cushion.
- Synovial Inflammation: The joint lining becomes irritated, producing enzymes that further “digest” healthy tissue.
- Mechanical Instability: A breakdown in the synchrony between muscles and ligaments, leading to abnormal joint “tracking”.
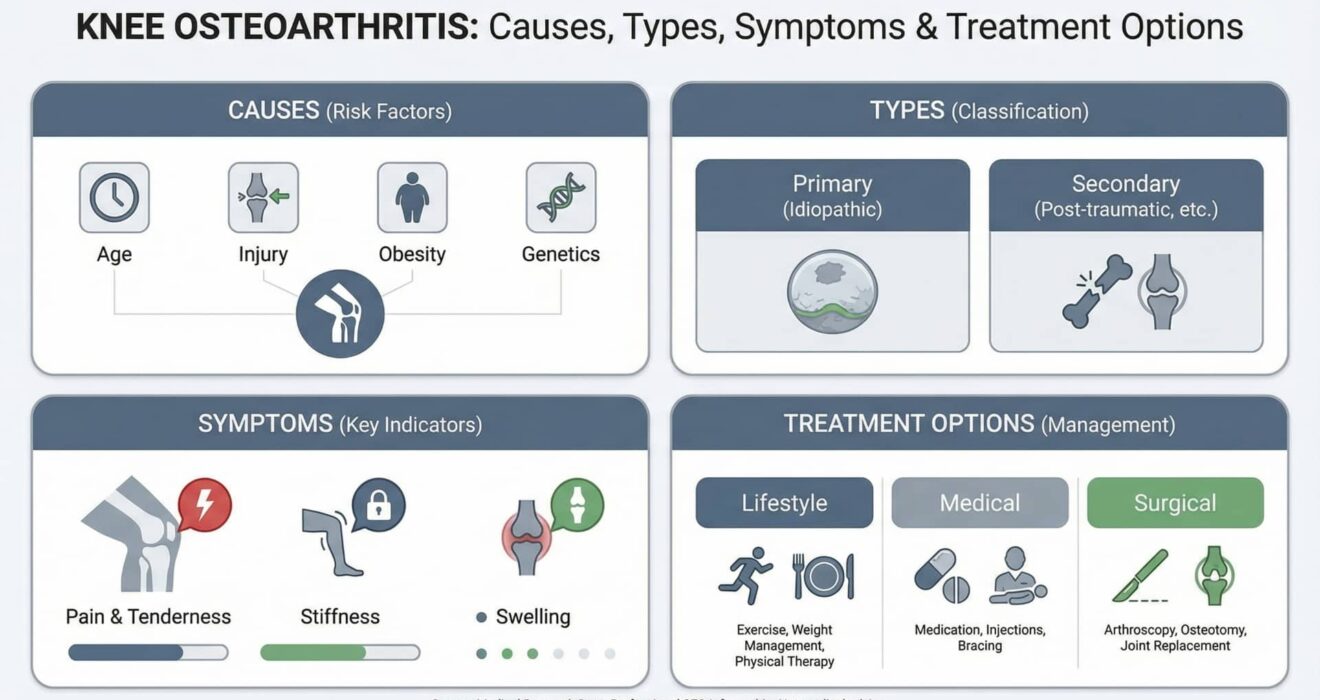
Causes of Knee Osteoarthritis: Why Joints Fail
Identifying the specific causes of knee osteoarthritis is the cornerstone of a “precision medicine” approach. If we can pinpoint why a joint is failing, we can better predict which treatments will yield the best results. We generally categorize these triggers into two primary groups.
Primary (Idiopathic) Osteoarthritis
- Cellular Senescence: As we age, our chondrocytes (cartilage cells) lose their “repair kit.” They become less efficient at maintaining the extracellular matrix, making the cartilage brittle and prone to fissuring.
- Genetic Predisposition: Your DNA largely dictates the robustness of your collagen fibers. Some individuals are genetically wired to produce higher levels of destructive enzymes (metalloproteinases) that prematurely break down the joint surface.
Secondary Osteoarthritis
Post-Traumatic OA (PTOA): The American Academy of Orthopedic Surgeons (AAOS) notes that joint fractures and high-grade sprains are major drivers of early OA. Even if a bone heals, the initial impact often causes “chondrocyte death” a loss of cells that can never be replaced.
Meniscal and ACL Injuries: The ACL and meniscus are the knee’s primary stabilizers. When a meniscus is torn or removed, the contact stress on the bone increases exponentially, often leading to rapid-onset arthritis in that specific compartment.
Obesity (The Metabolic Factor): While the mechanical load is a factor (during walking, the knee can experience several times your body weight in force, so even modest weight loss can meaningfully reduce knee load), the chemical factor is equally vital. Adipose (fat) tissue releases “adipokines” inflammatory chemicals that circulate in the blood and contribute to cartilage breakdown.
Biomechanical Malalignment: Issues like “bow-legs” (varus) or “knock-knees” (valgus) shift the body’s weight to one side of the knee, causing it to wear out significantly faster than the rest of the joint.
Pathophysiology: Structural Changes Within the Knee
To choose the right knee osteoarthritis treatment, one must visualize the structural changes occurring within the knee capsule. When hyaline cartilage thins, the joint loses its natural “lubrication.” The synovial fluid, which should be thick and protective like engine oil, becomes thin and watery.
The body attempts to stabilize the joint by producing new bone at the margins. These are osteophytes, or bone spurs. While the body intends for these to increase the surface area for weight-bearing, they usually result in restricted motion and “pinching” of surrounding soft tissues.
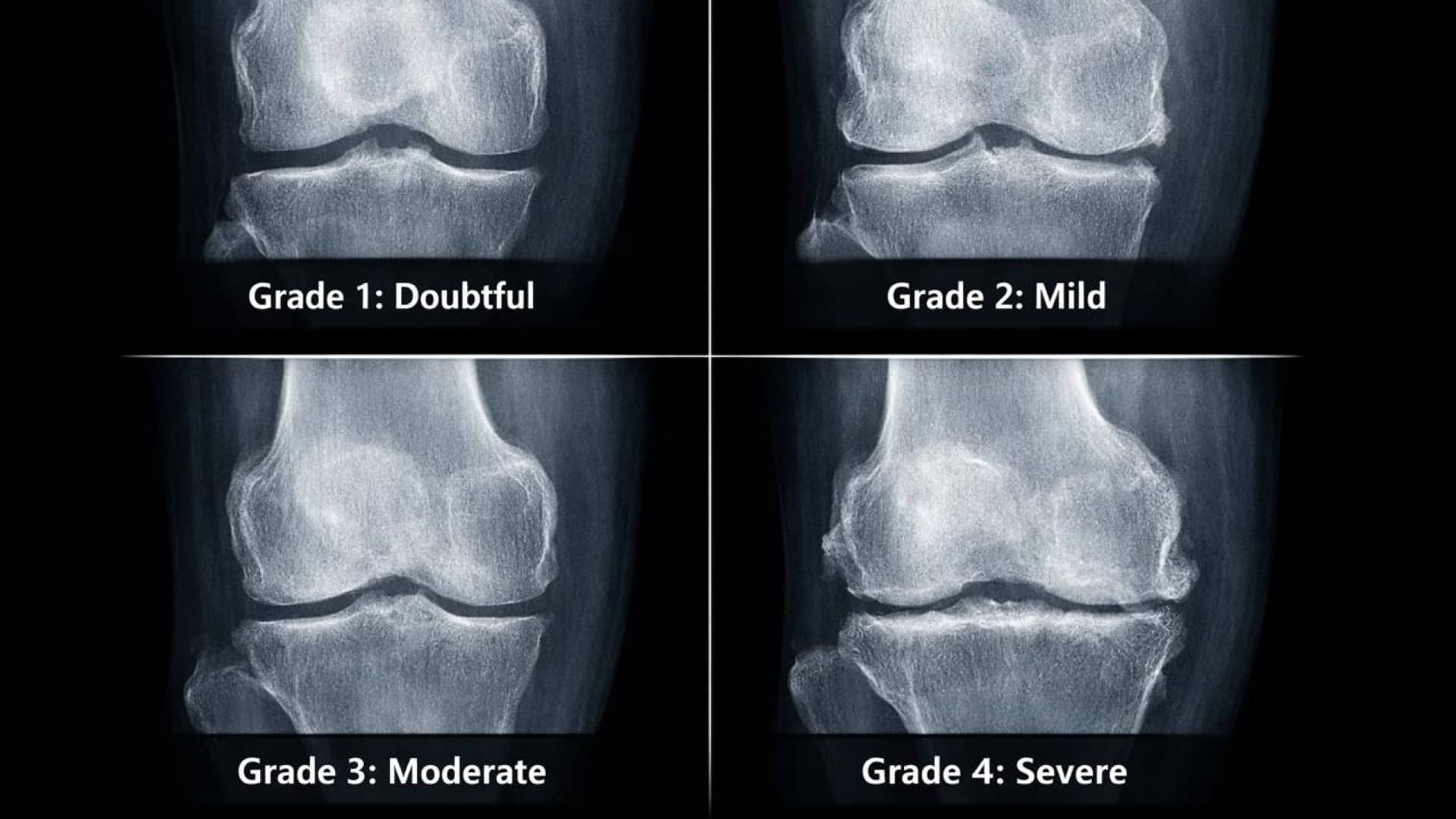
The Kellgren-Lawrence (K-L) Classification System
Orthopedic specialists use the K-L grading system to quantify this progression and determine the appropriate level of intervention:
- Grade 1 (Doubtful): Minimum bony lipping; the beginning of the process.
- Grade 2 (Mild): Definite bone spurs are present, but the “gap” between bones is still healthy.
- Grade 3 (Moderate): Moderate narrowing of the joint space. The bones are beginning to rub.
- Grade 4 (Severe): “Bone-on-bone” contact. Large spurs and significant hardening of the bone.
Knee Osteoarthritis Symptoms: Recognizing the Red Flags
The clinical presentation of OA is unique to every patient, but certain “red flags” are hallmarks of the disease.
Weight-Bearing Pain: Initially, the pain is “mechanical”: it hurts when you use it (such as climbing stairs) and improves with rest. In advanced stages, the pain becomes “inflammatory,” persisting even at night.
The 30-Minute Rule: Patients often feel “rusty” or “stuck” upon waking. Unlike systemic conditions like Rheumatoid Arthritis, which cause hours of stiffness, OA stiffness typically resolves within 20 to 30 minutes of movement.
Crepitus: This is the audible “crunching” or “grinding” sensation. It is the sound of irregular bone surfaces rubbing together without a smooth buffer.
Joint Effusion (Swelling): Commonly called “water on the knee,” this occurs when the lining of the joint becomes irritated and overproduces fluid, leading to a “tight” feeling that limits bending.
The “Theatre Sign”: A dull ache or stiffness that occurs after sitting for long periods (like at a movie or on a flight). This is a classic sign of involvement of the kneecap (patellofemoral) joint.
Orthopedic Insight: If your knee feels like it is “giving way,” it may not be a torn ligament. It is often a pain-inhibited reflex; your brain momentarily “shuts down” the quadriceps muscle to protect the joint from a painful movement.
For a broader perspective on systemic joint issues:👉 https://greatertxortho.com/understanding-joint-rheumatism/
Diagnosis: Beyond the Physical Exam
At GTOA, we treat the patient, not just the X-ray. A professional diagnosis involves a multi-modal approach:
Clinical Examination: We begin with a Gait Analysis to see how you compensate for the pain. We check for joint line tenderness and measure your Range of Motion (ROM). A loss of “extension” (the ability to fully straighten the leg) is often the first sign of significant joint change.
Weight-Bearing X-rays: This is the gold standard. X-rays taken while you are lying down are misleading; we need to see how the joint behaves under the actual pressure of your body weight.
MRI (Magnetic Resonance Imaging): While X-rays show bone, MRIs show the “soft” story. They are invaluable for detecting Bone Marrow Lesions (BMLs) areas of bruising inside the bone that are a significant source of pain and for evaluating the health of the menisci and ligaments.
Knee Osteoarthritis Treatment: The Step-Ladder Strategy
The goal of treatment is to manage symptoms and preserve function. We follow a “Step-Ladder” approach, moving from conservative to invasive only when necessary.
Conservative Management (The Foundation)
According to AAOS evidence-based guidelines, the most effective treatments are often the most accessible:
- Weight Management: Losing just one pound of body weight removes four pounds of pressure from the knee. It is one of the few interventions that directly reduces mechanical stress on the joint.
- Structured Physical Therapy: Strengthening the quadriceps and hamstrings acts as a “natural brace” for the knee.
- Unloader Bracing: Specialized braces can “shift” the pressure away from the damaged side of the knee, allowing for pain-free walking.
- Pharmacotherapy: We often recommend topical NSAIDs (creams) over oral pills for long-term use to reduce systemic side effects on the kidneys and stomach.
👉 Corrective Exercises for Knee Pain Relief

Injection Therapy (The “Bridge”)
When lifestyle changes aren’t enough, we look inside the joint:
Corticosteroids: These are powerful anti-inflammatories that “put out the fire” of a painful flare-up.
Viscosupplementation (Hyaluronic Acid): Often called a “gel shot,” this supplements the joint’s natural lubricant. It works best for Grade 2 and 3 patients.
PRP (Platelet-Rich Plasma): This regenerative therapy uses the patient’s own blood to deliver growth factors into the joint, reducing inflammation and may help improve the joint environment in selected patients.
Surgical Intervention (The Definitive Step)
When “bone-on-bone” pain dictates your life, modern surgery offers a remarkable return to function:
Partial Knee Replacement (UKR): If only one part of the knee is worn out, we replace only that part, preserving your natural ligaments and a “natural” feeling knee.
Total Knee Replacement (TKR): The gold standard for end-stage OA. Robotic-assisted techniques can support more consistent alignment and implant positioning, which may support more precise implant positioning and alignment.
The Importance of Early Intervention
The biggest risk in knee OA is the “Cycle of Deconditioning.” When the knee hurts, the patient stops moving; when they stop moving, the muscles atrophy; when the muscles atrophy, the joint loses its support and the arthritis gets worse.
By intervening early, we break this cycle. “Pre-hab” (strengthening before surgery) is the single best predictor of how well a patient will do after surgery. Furthermore, ignoring knee osteoarthritis symptoms can lead to “kinetic chain” issues, causing secondary pain in the hip and lower back as the body compensates for knee dysfunction.
Conclusion
Knee osteoarthritis is a progressive condition, but it is not a diagnosis of defeat. The field of orthopedics has moved into an era of “tailored” care. Whether you are a marathon runner looking for regenerative options or a grandparent wanting to walk in the park pain-free, there is a path forward.
Long-term mobility usually comes down to doing the basics well staying active, protecting the joint, and using the right treatment at the right time. By understanding the causes of knee osteoarthritis and acting on the symptoms today, you are investing in your mobility for the decades to come.
