CRPS After a Car Accident: Symptoms, Diagnosis, and Legal Impact
Complex regional pain syndrome (CRPS) is a chronic pain condition that can develop in a limb after trauma. In CRPS after car accident injuries, pain may intensify even as the original fracture, sprain, or soft tissue injury appears to heal. Patients may experience burning pain, swelling, sensitivity to touch, changes in skin color or temperature, and progressive loss of function.
For patients, the concern is understanding why recovery has stalled. For attorneys and legal teams, the concern is whether the medical record clearly documents the timeline, examination findings, functional limitations, and diagnostic reasoning that support a clinically recognized regional pain disorder.
This article explains how CRPS may develop after a collision, which symptoms require evaluation, how doctors reach a diagnosis, what treatment may involve, and why consistent documentation matters in injury claims.
Understanding CRPS after car accident trauma requires careful attention to the symptom timeline, physical findings, and changes in daily function.
Understanding CRPS After Car Accident Injuries
A driver rear-ended on I-10 in Houston braces against the steering wheel and fractures the distal radius. The fracture is casted and heals on schedule. Six weeks later, the cast comes off and the hand looks wrong: puffy, shiny, cooler than the other hand, and painful when a shirt sleeve brushes against it.
This pattern pain that persists, spreads, or becomes more severe than expected is characteristic of CRPS. The condition is associated with abnormal pain processing and changes involving the sensory, autonomic, vascular, and motor systems. Because the original injury may appear modest and early imaging may be reassuring, the condition can be overlooked during the first stages of recovery.
Complex Regional Pain Syndrome in Plain English
Based on Cleveland Clinic’s explanation, complex regional pain syndrome is a long-lasting pain condition, usually affecting one limb, that develops after an injury, surgery, stroke, or other event, and involves pain that is more severe and more persistent than the original injury would suggest.
Symptoms may not be fully recognizable immediately after the collision. In some patients, the pattern becomes clearer over the following days or weeks, particularly when pain, swelling, sensitivity, or temperature changes continue beyond the expected healing period.
Clinicians generally describe two forms. CRPS Type I occurs when no specific peripheral nerve injury is identified. CRPS Type II develops when there is evidence of an identifiable nerve injury. The symptoms and treatment approaches may overlap, but the distinction can matter when evaluating causation and selecting diagnostic tests.
Why It Feels Different From Normal Healing Pain
Ordinary post-injury pain fades as tissue repairs. It stays roughly where the injury was, it responds to rest, and it improves week over week.
This condition does the opposite. Pain often spreads beyond the injured structure, the limb may react to light touch or temperature changes, and function declines rather than improves. Patients frequently report that the limb no longer feels like it belongs to them, and many begin guarding it, which accelerates stiffness and weakness.
How a Crash Can Trigger CRPS
Motor vehicle trauma provides several plausible triggers, and no single mechanism explains every case. Reported inciting events include:
- Distal radius and wrist fractures from bracing against the wheel or dashboard
- Ankle and foot fractures from pedal or floorboard impact
- Crush injuries to the hand, foot, or forearm
- Surgical repair of a crash-related fracture
- Prolonged casting or immobilization of a limb
- Traction or stretch injury to a peripheral nerve
- Soft tissue trauma with no fracture at all
The severity of the initiating injury does not reliably predict who develops the syndrome. Minor trauma can precede a severe presentation, which is one reason the diagnosis draws scrutiny in injury claims.
Complex Regional Pain Syndrome Symptoms
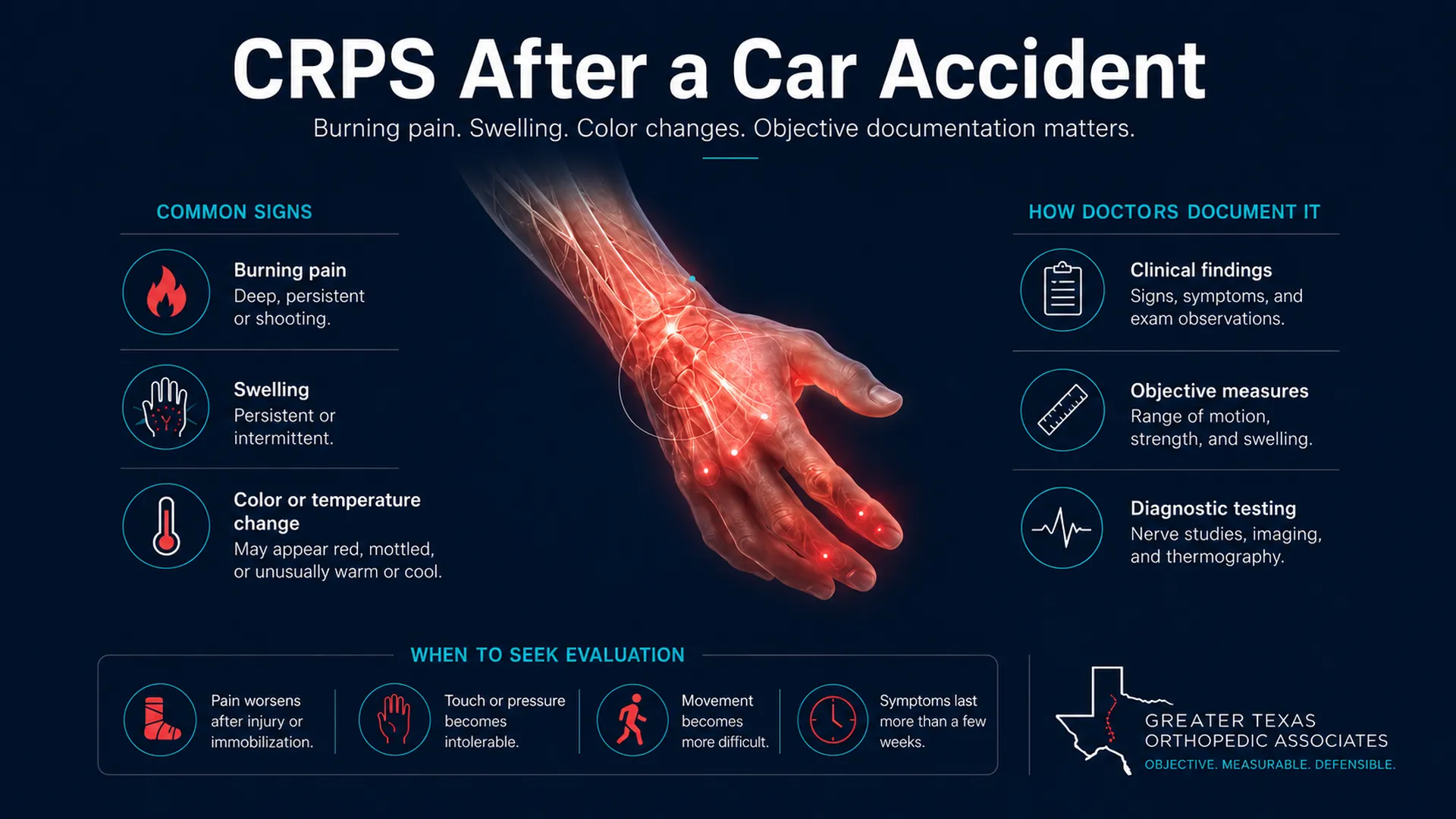
Complex regional pain syndrome symptoms often appear as a cluster rather than as one isolated complaint. Patients may experience burning, throbbing, or persistent aching pain, severe sensitivity to light touch or clothing, and pain that is greater than expected from the original injury.
Other findings may include persistent swelling in the hand, wrist, foot, or ankle; skin that appears red, pale, blue, or mottled; and temperature differences between the affected and unaffected limbs. Changes in sweating, hair, nails, or skin texture may also occur, along with stiffness, weakness, tremor, or reduced range of motion.
Symptoms can fluctuate, so one normal-looking appointment does not necessarily reflect the patient’s experience throughout the day.
Red Flags That Need Prompt Evaluation
Certain presentations warrant timely assessment rather than watchful waiting:
- Pain that intensifies after a cast or splint is removed instead of easing
- A limb that changes color or temperature compared with the other side
- Swelling that persists well past the expected healing window
- Inability to tolerate light touch on skin that was previously normal
- Progressive loss of motion, grip strength, or weight-bearing tolerance
- New tremor, jerking, or a limb that will not move on command
Severe pain with tightness, numbness, and pallor in the early hours after trauma is a separate emergency and may point to compartment syndrome, which requires immediate care.
How Doctors Reach a CRPS Diagnosis After Injury
A CRPS diagnosis after injury cannot be established by pain severity alone. Physicians evaluate the symptom history, observable examination findings, timing of onset, and whether another medical condition could better explain the changes in the affected limb.
There is no single blood test or scan that confirms this condition. It remains a clinical diagnosis, built from history, examination, and the exclusion of alternatives. That reality shapes both the medical pathway and the legal one.
How the Budapest Criteria Support a CRPS Diagnosis
Physicians commonly use the Budapest Criteria when evaluating suspected CRPS. These criteria require continuing pain that is disproportionate to the original injury, patient-reported symptoms in several clinical categories, and observable signs during the examination. The four categories include sensory changes, vasomotor changes, swelling or sweating abnormalities, and motor or tissue changes. The physician must also determine that no other diagnosis better explains the findings.
Examiners may measure limb temperature and circumference side to side, test light touch and pinprick sensitivity, grade grip or weight-bearing capacity, photograph color changes, and repeat these measures over time. Serial documentation matters here more than in most orthopedic conditions, because the findings vary. Recorded this way, objective medical findings turn a fluctuating complaint into a measured, dated, reproducible record.

What Imaging and Testing May Show
Imaging and diagnostic testing may support the evaluation or help rule out other causes, but no scan independently confirms CRPS. A normal MRI does not exclude the condition. X-rays may show bone changes in some longer-standing cases, while EMG and nerve conduction studies may help identify a peripheral nerve injury or exclude conditions such as radiculopathy. Bone scans or temperature measurements may occasionally be used in selected cases, but the diagnosis remains primarily clinical.
Sympathetic nerve blocks may be used to reduce pain and help a patient participate in therapy. A temporary response may provide useful clinical information, but it does not independently confirm or exclude CRPS.
Causation, Pre-Existing Pain, and Delayed Onset
In injury claims, causation often depends on four elements: a documented mechanism of injury, a medically plausible timeline, examination findings that correspond with the reported symptoms, and consideration of other possible causes.
Prior neuropathy, diabetes, chronic pain, or an earlier limb injury does not automatically exclude a crash-related diagnosis. However, the treating physician should explain whether the collision caused a new condition, aggravated a pre-existing problem, or is unrelated to the current findings. Alternative diagnoses may include infection, deep vein thrombosis, an unrecognized fracture, radiculopathy, or peripheral neuropathy.
Treatment Options for CRPS
AAOS explains that early treatment tends to produce better outcomes, and most protocols prioritize restoring movement rather than resting the limb. A typical progression includes:
- Physical and occupational therapy focused on desensitization, graded movement, and functional use of the limb
- Medications used for neuropathic pain, along with anti-inflammatory or bone-targeted agents in selected cases
- Sympathetic nerve blocks and other image-guided procedures when pain limits participation in therapy
- Psychological support and pain coping strategies, since fear of movement can drive disuse and stiffness
- Neuromodulation, such as spinal cord stimulation, considered for cases that do not respond to conservative care
Outcomes vary. Some patients improve substantially, particularly when the condition is recognized early, while others develop persistent pain and lasting functional limitations. Treatment records should track changes in movement, strength, daily activity, and work capacity rather than relying only on pain scores. Gaps in care may affect both recovery and documentation, because prolonged inactivity can worsen stiffness while unexplained interruptions can make the clinical timeline harder to evaluate.
What a CRPS Legal Claim Requires From the Medical Record
In a chronic pain syndrome legal claim involving CRPS, the medical record often carries more weight than any single imaging study. Because the condition may produce significant disability without a dramatic scan, a defensible record should clearly document the injury mechanism, symptom timeline, examination findings, functional limitations, and treatment plan.
- The mechanism of injury and the date, tied to the collision
- The first documented complaint of disproportionate pain and its date
- Serial exam findings with measured values, not adjectives
- Photographs or measurements of color, swelling, and temperature asymmetry
- The clinical criteria applied and how the patient met them
- Response to sympathetic blocks or other targeted interventions
- Functional limits stated in concrete terms: grip capacity, weight-bearing tolerance, hours of hand use, driving, work duties
- A treatment plan with anticipated future care needs
At Greater Texas Orthopedic Associates, pain management physicians, including Dr. John Hall, evaluate persistent post-traumatic limb pain and document relevant examination findings, diagnostic reasoning, functional limitations, and treatment recommendations.
When to Schedule an Orthopedic Evaluation
An orthopedic or pain management evaluation may be appropriate when limb pain worsens instead of improving, the affected limb differs in color or temperature from the opposite side, or a healed fracture leaves continuing loss of function. Evaluation is also reasonable when persistent symptoms have been attributed to anxiety or deconditioning without a detailed examination for sensory, vascular, swelling, and motor changes. In suspected CRPS after car accident cases, early evaluation can help document the symptom pattern before findings change or become less obvious.
Earlier assessment can support treatment and reduce gaps in the medical timeline.
FAQs About CRPS After a Car Accident
How soon after a crash can symptoms begin?
Symptoms commonly appear within days to several weeks of the trauma or of a related surgery. A later onset does not rule out the diagnosis, though it does raise the value of documenting what changed and when.
Can it develop without a fracture?
Yes. Sprains, crush injuries, and soft tissue trauma with no fracture have all been reported as triggers. Injury severity is a poor predictor of who develops the syndrome.
Does a normal MRI mean the pain is not real?
No. Standard imaging is frequently normal in this condition. The diagnosis rests on clinical criteria and examination findings, not on a scan result.
How is CRPS diagnosed after an injury?
Doctors generally diagnose CRPS through medical history, physical examination, and clinical criteria. They evaluate sensory changes, temperature or color differences, swelling or sweating abnormalities, and changes in movement or tissue condition. Testing may help exclude other causes, but no single scan confirms CRPS.
Which specialist should evaluate it?
An orthopedic or pain management physician experienced with post-traumatic neuropathic pain is generally the right starting point, with neurology or neurosurgery involved when a nerve injury is suspected.
Final Thoughts
CRPS after car accident injuries can turn a seemingly limited limb injury into a persistent pain and mobility problem. Warning signs include burning pain, touch sensitivity, swelling, changes in skin color or temperature, and function that declines instead of improving.
Patients experiencing these changes should seek evaluation rather than waiting for the symptoms to resolve on their own. Greater Texas Orthopedic Associates can assess persistent post-traumatic limb pain, document the relevant findings, and recommend an appropriate treatment plan.
This article is for educational purposes and is not a substitute for individual medical evaluation.