How Diagnostic Injections Help Prove Pain in Injury Cases
After a serious crash, real pain does not always show up clearly on imaging. A patient may have constant neck or back pain, an MRI that looks unremarkable, and a growing fear that no one believes how much they hurt. In personal injury case workups, diagnostic injections can help close this gap because they answer a specific clinical question instead of relying on a picture alone.
For patients, the concern is why the pain has no obvious explanation on a scan. For attorneys, case managers, and legal teams, the concern is whether the medical record connects symptoms, crash mechanism, exam findings, the injection response, and treatment need.
This kind of injection is not the same as a routine pain shot. It is designed to identify or rule out a specific pain source by numbing one targeted structure and measuring how the pain responds. That measured response can become an important objective finding in an injury claim.
Diagnostic Injections in Injury Cases: Why a Targeted Test Matters
A driver rear-ended at a red light in Houston may walk away from the crash, then develop deep neck and shoulder pain over the following week. Her MRI shows no herniated disc and no fracture, and an insurance reviewer questions whether she was really hurt. The pain is real, but the imaging alone cannot explain where it begins.
This is the situation a targeted injection is built for. Instead of relying on a picture, the physician tests the pain directly. The result becomes part of the objective findings that support an injury case and helps connect symptoms to a specific anatomical source.
When the test confirms the source, the next step in treatment becomes clearer. When the test is negative, the care team also learns something useful and looks elsewhere.
What a Diagnostic Injection Means in Plain English
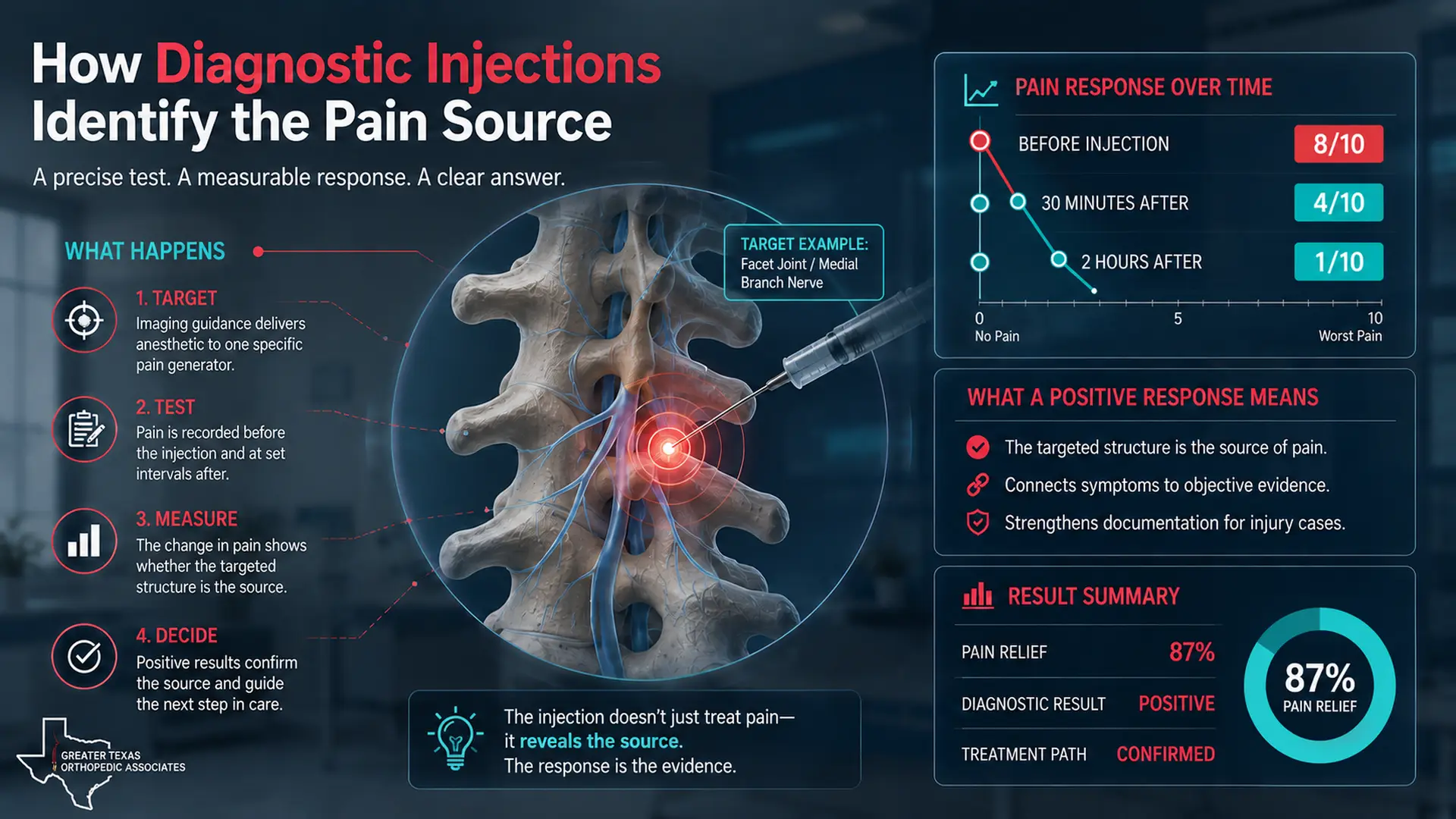
It delivers a small amount of numbing medication, usually a local anesthetic, into or near one specific structure under image guidance. The patient then records how much the pain changes over the next several hours.
Based on Cleveland Clinic’s explanation, facet joint pain and nerve-related pain can be difficult to identify from imaging alone, which is why targeted injections may be used to clarify the source. The injection is mainly a test. Any pain relief it produces during that window is the data the physician uses to interpret the result.
Why It Feels Different From a Routine Pain Shot
A routine therapeutic injection is meant mostly to reduce pain over weeks. The diagnostic version is meant to produce information. The response is recorded in measurable terms, often as a percentage of relief along with pain scores before and after. The shorter, more specific reaction is exactly what makes the test useful for documentation.
How Diagnostic Injections Help Identify the Pain Source
The procedure is performed with fluoroscopy or ultrasound so the medication reaches the targeted structure and not nearby tissue. The patient then logs their pain at set intervals while the anesthetic is active.
Common steps that make the test meaningful include:
- Image guidance to place medication into a single specific structure.
- A pain score recorded before the injection.
- Pain scores recorded again at one, two, and several hours after.
- A documented percentage of relief during the anesthetic window.
- A repeat block on a separate day to confirm a strong first response.
- A clear note explaining what the result means for the next step in care.
A sharp, time-limited reduction in pain supports that the targeted structure is a real source. No change in pain points the workup elsewhere.
Symptoms That May Call for a Targeted Injection
Not every patient needs a targeted injection. The test is most useful when pain persists despite reasonable conservative care, when imaging does not explain the symptoms, or when the pattern of pain suggests a joint or nerve source that cannot be confirmed any other way.
When Persistent Pain After a Crash Matters
Symptoms that may justify consideration of a targeted injection include:
- Neck or back pain lasting several weeks or more after a collision.
- Pain that worsens with specific motions such as extension, rotation, or twisting.
- Pain in a known facet or nerve distribution despite a normal MRI.
- Limited improvement from physical therapy and oral medication.
- Recurrent flare ups during work, driving, or sleep.
These patterns deserve a focused evaluation, not another round of generic pain control. Identifying the source early shapes what treatment can realistically achieve.
Facet Injections and Medial Branch Blocks in Spinal Injury Cases
Two of the most common spinal versions of this test are the facet injection and the medial branch block. Both target the same pain pathway from a different direction, and both are widely used after motor vehicle and workplace injuries.
Facet Injections Personal Injury Case Use
The facet joints are small paired joints at the back of the spine that guide and limit motion. A facet injection places a small amount of anesthetic, sometimes combined with a steroid, into or around the joint. In a personal injury case, a facet injection finding becomes meaningful when the patient reports a clear drop in pain during the anesthetic window. That response supports the facet joint as the pain generator and not a disc or muscle.
Medial Branch Blocks in Personal Injury Documentation
The medial branch nerves are the small nerves that carry pain signals away from each facet joint. A medial branch block personal injury workup numbs those nerves rather than the joint itself. Two separate blocks performed days apart, each producing strong temporary relief, is considered a more reliable confirmation that the joint is the source. Based on AAOS information on spinal pain procedures, this kind of structured testing can guide further treatment decisions, including longer term nerve targeted care.
Why Imaging Alone Cannot Replace These Tools
MRI and CT show structure. They do not show pain. A facet joint can look normal on imaging and still be the source of disabling symptoms, especially after a sudden jolt from a rear impact. A targeted injection can be one of the most direct ways to test that link. Coordinated medial branch block evaluations can give the medical record a measurable, time-stamped result that imaging alone cannot provide.
Causation, Pre Existing Findings, and Accident-Related Pain
Causation questions come up almost every time imaging shows pre existing degeneration. Defense reviewers may argue that the findings predate the crash and that current pain reflects age, not injury. A documented positive injection result complicates that argument because it shows the joint or nerve is producing pain now, in a way that matches symptoms that began after the collision.
GTOA’s discussion of orthopedic causation in personal injury cases explains how mechanism, symptom timing, exam findings, and treatment response work together to clarify whether new pain is accident-related. A positive injection result adds another verifiable point on that timeline.

How the Injection Result Guides Treatment
A confirmed result rarely ends the story. Once a source is confirmed, treatment is built around that exact structure. A patient who responds clearly to medial branch blocks becomes a stronger candidate for radiofrequency ablation, a procedure that calms the same nerves for a much longer period. A patient whose pain comes from a different structure avoids unnecessary procedures and can be redirected to therapy or surgical consultation that fits the real source.
Treatment that may follow a confirmed result includes:
- Targeted physical therapy focused on the specific joint or movement pattern.
- Image-guided therapeutic injections to reduce inflammation at the confirmed source.
- Radiofrequency ablation after two positive medial branch blocks.
- Continued pain management while function is restored.
- Surgical referral when structural damage and severe symptoms support it.
The strongest treatment plans match the documented finding instead of guessing at the source.
Why Documentation Matters for Patients and Attorneys
This test is one of the few orthopedic evaluations where the patient’s pain is measured in real time, before and after a targeted intervention. That measurement becomes part of the medical record and can be reviewed later by any reader, including a defense expert or an insurance adjuster.
Pain management in personal injury cases gains real credibility when injections are part of a structured workup, with image guidance, recorded pain scores, and clear conclusions. Coordinated pain management and interventional care helps connect the patient’s symptoms, the targeted injection, the measured response, and the resulting treatment plan into one consistent record.
Documentation should describe the injection target, the imaging used to confirm placement, the medication delivered, pain scores at recorded intervals, the percentage of relief reported, and the conclusion drawn from the result. A vague note such as “had injection, felt better” does not carry the same weight as a structured record showing a specific drop in pain at specific time points.
When to Schedule an Orthopedic or Pain Management Evaluation
A patient should consider evaluation when neck or back pain continues several weeks after a crash, when imaging does not explain ongoing symptoms, or when conservative care has not produced meaningful progress. Targeted injections are not the first step in most cases, but they are an important option once simpler treatment has failed to identify or relieve the source of pain.
For attorneys and case managers, referral may be appropriate when the existing record does not explain why pain has persisted, where it is coming from, or what the next medical step should be. A focused orthopedic evaluation for accident-related pain can consider whether a targeted injection is appropriate, document the result, and connect the finding to a treatment plan that fits the injury.
Final Thoughts
Diagnostic injections personal injury case workups give physicians a precise way to identify the source of pain when imaging falls short. By numbing one targeted structure and measuring how the pain responds, the test produces something the medical record can stand on. That kind of measurable evidence supports treatment decisions, and it helps attorneys and case managers explain why specific care was medically necessary after a crash.
When neck or back pain continues after an accident and the cause is unclear, Greater Texas Orthopedic Associates can evaluate the symptoms, consider whether a targeted injection is appropriate, document the response, and guide the next step in care.
Note: This article is intended for general informational purposes and does not constitute medical or legal advice. Patients should consult a qualified healthcare provider for evaluation and treatment of any injury.
FAQs About Diagnostic Injections in Injury Cases
What is a diagnostic injection in a personal injury case?
A diagnostic injection is a targeted procedure used to help identify whether a specific joint, nerve, or pain pathway is contributing to a patient’s symptoms. By placing numbing medication near a suspected pain source and recording pain levels before and after the injection, the physician can gather objective information that supports diagnosis, treatment planning, and injury documentation.
How can diagnostic injections help document pain after an accident?
Diagnostic injections can help document pain by showing how symptoms respond when a specific structure is temporarily numbed. If the patient reports a clear, time-limited reduction in pain during the expected anesthetic window, that response may support the suspected pain source and provide a measurable finding within the medical record.
Are diagnostic injections the same as regular pain injections?
No. A regular therapeutic injection is mainly intended to reduce pain over time. A diagnostic injection is primarily used to answer a clinical question: where is the pain coming from? Any temporary relief is measured and documented to help guide the next step in care.
Why are medial branch blocks sometimes done more than once?
Medial branch blocks may be repeated because a single response may not be enough to confirm the pain source. When two separate blocks produce strong, temporary relief, the result can provide stronger clinical support that the facet joint pain pathway is involved and may help guide treatment options such as radiofrequency ablation when appropriate.
Can diagnostic injections help when an MRI does not clearly explain the pain?
Yes. Imaging can show structural findings, but it does not always show where pain is coming from. A diagnostic injection can help test a suspected pain source directly. This can be especially useful when symptoms, exam findings, and imaging do not fully explain ongoing neck or back pain after an accident.