
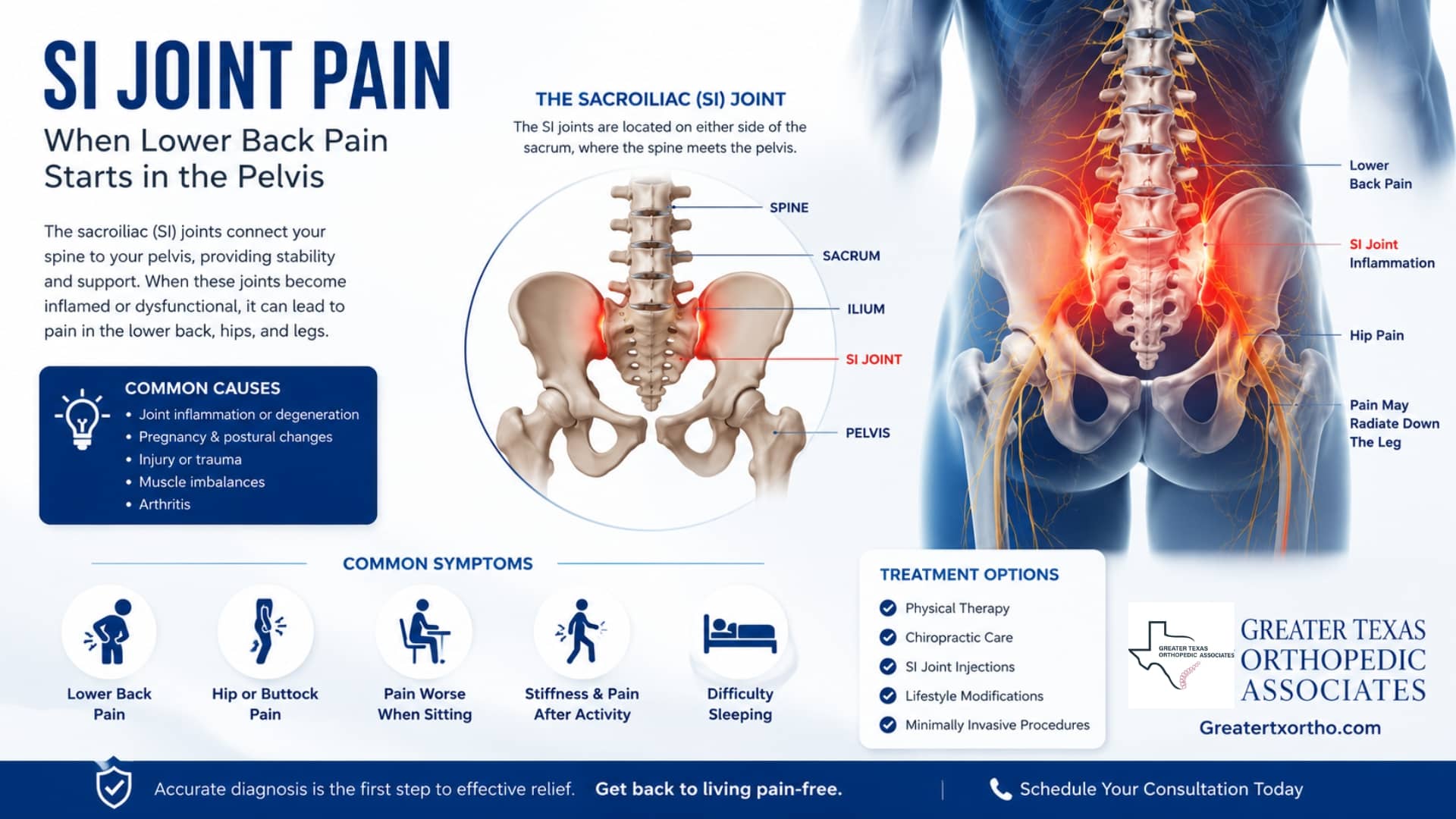
SI Joint Pain: When Lower Back Pain Starts in the Pelvis
SI joint pain is a common but often overlooked cause of lower back, buttock, hip, or groin pain. The sacroiliac joint connects the lower spine to the pelvis, and when it becomes irritated or overloaded, symptoms can feel very similar to a lumbar disc problem, sciatica, or hip condition.
For patients recovering from an accident, repetitive strain, or chronic pelvic instability, identifying the true source of pain is essential. A focused orthopedic or pain management evaluation can help determine whether symptoms are coming from the SI joint, lumbar spine, hip, or a combination of structures, leading to a more accurate diagnosis and targeted treatment plan.
Why SI Joint Pain Can Mimic Ordinary Lower Back Pain
The sacroiliac joint connects the sacrum at the base of the spine to the ilium of the pelvis. It does not move like a shoulder or knee. Its motion is small, but its job is substantial: absorbing load, transferring force, and helping stabilize the body when you stand, walk, climb stairs, or rise from a chair.
That is why lower back pain from pelvis mechanics can be so confusing. The painful area may sit near the beltline, deep in the buttock, or slightly off to one side. Some patients feel it after sitting too long. Others notice a sharp catch when rolling in bed, stepping out of a car, or putting weight through one leg.
Why a Small SI Joint Problem Can Cause Significant Pain
A healthy sacroiliac joint is stiff enough to support the upper body but flexible enough to tolerate daily movement. Trouble starts when the joint becomes inflamed, strained, unstable, or overloaded by changes elsewhere in the body. After trauma, even a subtle shift in walking pattern can keep stressing the area.
In clinical practice, sacroiliac joint pain is often considered when symptoms are one-sided, sit below the lumbar spine, and do not fit neatly with a disc or nerve-root pattern.

Common Causes of SI Joint Pain
SI joint pain can begin suddenly after an injury or develop gradually as the body compensates for another problem. A patient with hip pain may change how they walk. A worker with repeated lifting may load one side harder than the other. A driver hit from behind may develop pelvic and lumbar irritation at the same time. In many of these cases, sacroiliac joint pain develops because abnormal force continues stressing the pelvic joints and surrounding ligaments.
Several patterns raise suspicion:
- Pain beginning after a motor vehicle collision, fall, lifting incident, or sudden twisting motion.
- Discomfort that worsens with stairs, standing on one leg, getting out of a chair, or turning in bed.
- Aching near the posterior pelvis, buttock, hip, or groin rather than only in the center of the spine.
- Symptoms that improve briefly with rest but return when normal activity resumes.
- Prior lumbar, hip, or gait problems that may increase stress across the pelvic ring.
That is why a detailed history is clinically important, especially after an accident. For accident-related cases, documenting when the pain started, what movements reproduce it, and how function changed can guide treatment and support a clearer medical record.
SI joint pain symptoms that patients often overlook
SI joint pain symptoms can be subtle at first. Many people describe a deep ache on one side of the low back, close to the dimples of the pelvis. The pain may spread into the buttock, outer hip, groin, or upper thigh. Sacroiliac joint pain may feel sharp during transitions and dull after prolonged sitting or standing.
Some patients say, “It feels like my back is out,” but the most painful spot is not actually in the center of the lumbar spine. Others report that the first few steps after standing are the worst, then movement loosens things slightly before pain returns later in the day.
How it differs from a disc problem
Disc-related pain often follows a clearer nerve pathway, especially when there is numbness, tingling, weakness, or pain traveling below the knee. Sacroiliac irritation may refer pain into the leg, but it usually behaves more like mechanical pelvic pain than classic sciatica.
This difference becomes important when deciding whether treatment should focus on the spine, pelvis, or both. If the exam points toward the pelvis, a treatment plan focused only on the lumbar discs may miss the main driver.
When SI Joint Pain Symptoms Need Medical Evaluation
Pain after a significant accident, pain that keeps worsening, or pain that limits walking, work, or sleep deserves medical attention. New weakness, bowel or bladder changes, fever, unexplained weight loss, or severe progressive nerve symptoms should be evaluated urgently.
For less dramatic but persistent cases, the key is not to wait until the pain has shaped every movement pattern. Earlier evaluation can prevent a short-term joint irritation from becoming a long-term compensation problem.
How specialists evaluate pain that may start in the pelvis
A strong evaluation starts with a detailed history and a physical exam that tests the most likely pain sources. The clinician looks at where the pain sits, what provokes it, how the hips and lumbar spine move, and whether neurological findings suggest a different source. Provocative maneuvers may stress the sacroiliac joint to see whether they reproduce familiar pain.
Common Physical Exam Tests for SI Joint Pain
Several physical exam maneuvers can help clinicians determine whether the sacroiliac joint is contributing to a patient’s pain. No single test confirms sacroiliac joint pain on its own, but a combination of positive findings increases clinical suspicion.
Commonly used SI joint tests include:
- FABER test (Flexion, Abduction, External Rotation), which may reproduce pain near the posterior pelvis or groin.
- Thigh thrust test, where controlled pressure through the femur stresses the SI joint to identify pain reproduction.
- Compression and distraction tests, which apply force across the pelvis to evaluate joint irritation or instability.
- Gaenslen’s test, which places rotational stress across the pelvis and SI joint region.
When several of these maneuvers reproduce the patient’s familiar pain pattern, the SI joint becomes a more likely pain source.
Imaging can help rule out fractures, severe degeneration, inflammatory disease, or other structural problems, but it does not always prove the SI joint is the pain source. In selected cases, image-guided diagnostic injections can be useful because meaningful temporary relief after numbing the joint supports the diagnosis.
At GTOA, patients with persistent back, hip, and pelvic pain may be evaluated through orthopedic evaluations and coordinated with pain management when interventional options are appropriate.
Treatment options: from stabilization to targeted procedures
The right plan depends on severity, duration, exam findings, and whether the pain is mostly mechanical, inflammatory, post-traumatic, or part of a broader spine or hip problem. Most patients start with conservative care, then move to targeted interventions only when symptoms and function justify that step.
Early care may include:
- Activity modification that avoids repeated one-sided loading while keeping the patient moving safely.
- Physical therapy focused on pelvic stability, hip strength, gluteal control, and core coordination.
- Anti-inflammatory strategies when medically appropriate and cleared by the treating clinician.
- Bracing in selected cases where temporary external support helps calm painful motion.
- Image-guided injections when diagnosis or pain control requires a more targeted approach.
For persistent sacroiliac joint pain, treatment should focus on identifying the actual pain source, reducing irritation, restoring function, and preventing repeated stress on the joint. Conservative treatment for sacroiliac joint pain often includes physical therapy, pelvic stabilization exercises, activity modification, and image-guided injections when appropriate.
Where injections fit
An SI joint injection may be used diagnostically, therapeutically, or both. The diagnostic value comes from comparing pain before and after local anesthetic. The therapeutic value may come from reducing inflammation around the irritated joint.
Patients who also have radiating lumbar symptoms may need a broader spine evaluation. In some cases, services such as epidural steroid injections or facet joint injections are considered for different pain generators, which is why diagnosis should come before procedure selection.
Why accurate diagnosis matters after an accident
After a collision or fall, pain sources often overlap. A person may have lumbar strain, hip irritation, and lower back pain from pelvis dysfunction at the same time. If treatment focuses only on the most obvious symptom, another pain source may continue to slow recovery.
This is especially important in personal injury care. Clear documentation connects the patient’s complaints, exam findings, functional limitations, imaging, treatment response, and medical necessity. It also helps distinguish sacroiliac joint pain from other causes of post-traumatic back and hip pain.
For example, a patient rear-ended at a stoplight may first report “low back pain.” Two weeks later, the pain is mostly one-sided, worse when climbing stairs, and centered near the back of the pelvis. That pattern changes the clinical question for SI joint pain. The issue may not be only lumbar strain; it may be lower back pain from pelvis mechanics that needs a more specific exam and plan.
When to Take SI Joint Pain Seriously
SI joint pain is easy to underestimate because it hides inside a familiar complaint: lower back pain. But when pain starts near the pelvis, worsens with transitions, and refuses to behave like a straightforward disc or muscle problem, sacroiliac joint pain deserves a closer look.
Treatment works best when sacroiliac joint pain is diagnosed accurately and managed with a targeted plan focused on the true pain generator. That means careful evaluation, practical rehabilitation, selective use of image-guided procedures, and documentation that tells the full clinical story. If SI joint pain symptoms are disrupting work, sleep, walking, or recovery after an injury, a focused orthopedic and pain management evaluation can help clarify the next step.
For patients and legal teams needing coordinated care in Texas, contact GTOA to discuss evaluation options and the most appropriate path forward.

